首页
公司简介
乐动在线
不锈钢件加工
铝件加工
铅/黄铜件加工
零部件加工
设备展示
新闻资讯
公司新闻
行业新闻
加工知识
联系乐动(中国)
乐动在线
24小时服务电话:18600656293
乐动在线
引领机械加工行业
业务范围
乐动在线加工项目:精密加工,机械零件加工,非标定制以及批量加工!
服务优势
乐动在线优势:加工时间短、收费合理、设备先进,经验丰富。
服务能力
“24小时服务”,已为数万家客户提供机械加工服务,拥有专属厂房、办公和齐全的加工设备
乐动在线
乐动(中国)
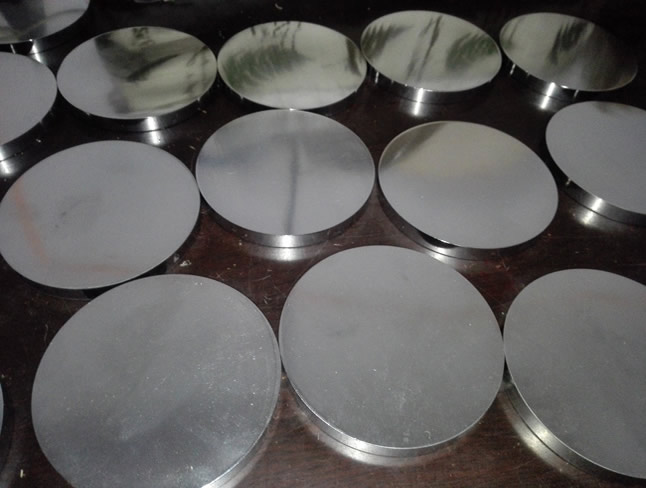
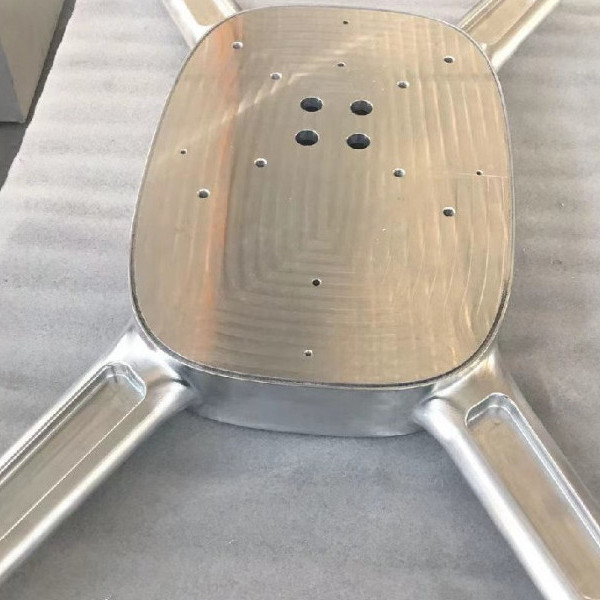
精密加工件
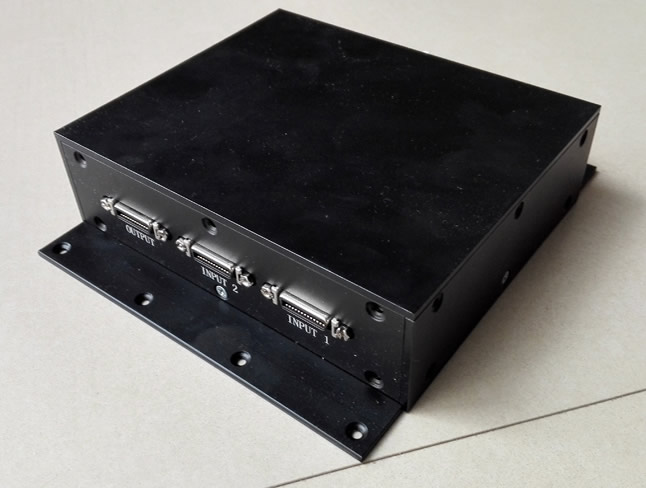
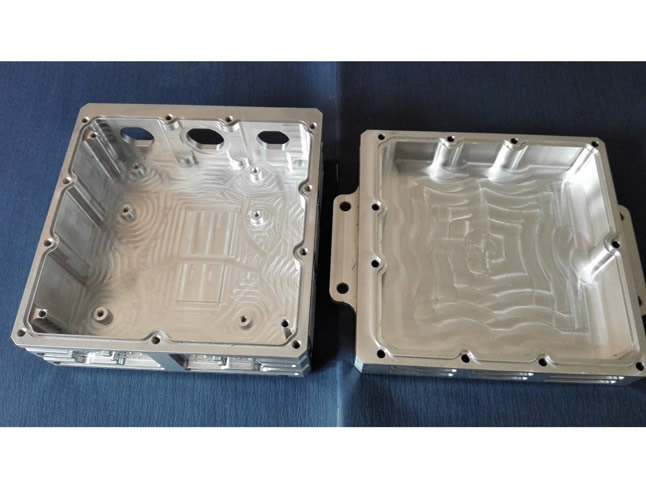
壳体加工件
乐动在线
加工件
加工件
壳体加工件
乐动在线
服务过的客户
行业资讯
乐动在线CNC铝合金机加工展示
2023-03-27
more
27
2023-03
乐动在线该如何选
27
2023-03
乐动在线CNC铝合金机加工展示
11
2022-02
乐动在线都支持哪些材料的零件加工?
11
2022-02
如何确定使用哪种加工工艺来实现高度可重复的零件
乐竞体育(中国)官方网站app
|
乐动在线
|
安博(中国)官方网站
|
乐动网页版登录入口
|
球友会·体育(中国)官方网站
|
华球体育
|
星空体育(China)官方网站
|
开云网页版
|
华体买球
|